Inguinal region
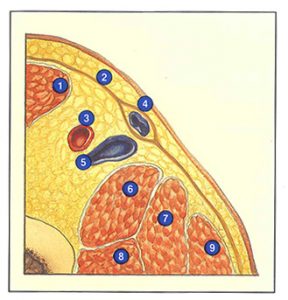
A transverse section of the inguinal region (Figure 60-A) reveals, from lateral to medial: the sartorius muscle (M. sartorius), the femoral artery just before giving rise to the arteria profunda femoris, the femoral vein, the termination of the long saphenous vein inside its aponeurotic sheath, and f nally, the adductor longus muscle (M. adductor longus ).
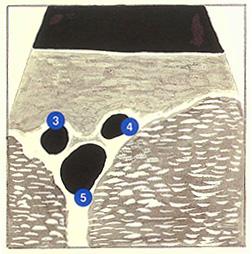
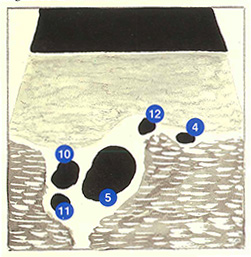
The ultrasonographic appearance is typical at this level (Figure 60-B). On transverse sections, with the transducer placed along the inguinal fold, a “Mickey Mouse” appearance is observed. The femoral vein (10 to 15 mm in diameter) forms the face, and the femoral artery (6 mm) and long saphenous vein (3 to 5 mm) form the two ears.
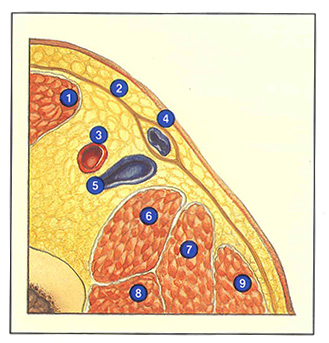
During ultrasound investigation, the transducer is then displaced distally. The long saphenous trunk becomes separated from the femoral vein by “rolling” over adductor longus muscle (Figure 60-C). An anterior branch is sometimes observed anterior to the long saphenous trunk. The femoral and profunda femoris arteries are observed posteriorly and laterally.
Ultrasound examination of this region must determine the diameter of the saphenofemoral junction, detect any anatomical variation of the saphenofemoral junction and, in the case of reflux, specify its origin.
Only minor variations of the diameter of the saphenofemoral junction are observed in healthy subjects. Depending on the phase of the menstrual cycle or the duration of standing prior to the examination, its diameter varies between 3 and 5 mm.
In contrast, all types of anatomical variants are common (see Volume 1). For example, the external pudendal artery sometimes occupies the saphenofemoral angle or, more rarely, passes in front of the saphenofemoral junction.
Finally, when reflux is detected by Doppler examination on the long saphenous trunk, five possible origins can be attributed in the inguinal region. The most common site of reflux is a lesion of the saphenous ostial valve at the saphenofemoral junction. More rarely, this valve is perfectly competent and reflux is derived from a tributary of the saphenofemoral junction (see Volume 1). In other cases, reflux arises from a proximal perforating vein, an accessory saphenous vein, or even a perineal network.
Further reading
Henriet J.P. Le confluent veineux saphéno-fémoral et le réseau artériel honteux externe : données anatomiques et statistiques nouvelles. Phlébologie 1987; 40: 711-35.
Vin E, Schadeck M. La maladie veineuse superficielle. Masson Ed, Paris, 1990.