Below the popliteal fossa
Two types of perforating vein can be distinguished below the popliteal fossa:
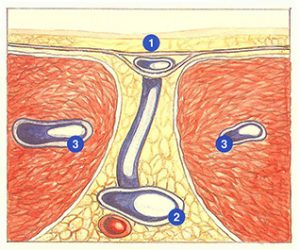
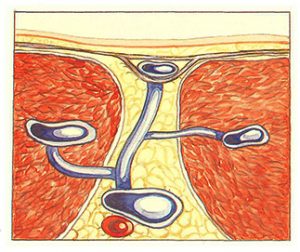
- Perforating veins not related to intramuscular veins: they directly connect superficial veins with deep intermuscular veins (anterior or posterior tibial veins, peroneal veins, and tibioperoneal trunk) (Figure 97);
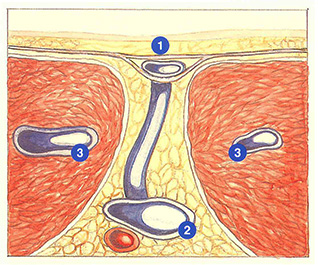
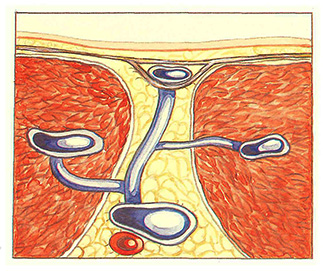
- Perforating veins connected to intrainuscular veins: they connect superficial veins with gastrocnemius or soleus veins (Figure 98)and often have multiple branches. connecting superficial, intermuscular. and intramuscular networks.
There are also transgastrocnemius perforating veins of the soleus muscle, which connect a superficial vein and veins of the medial head of the gastrocneniius muscle and the soleus muscle.
Functionally, direct perforating veins not related to intramuscular veins constitute a safety valve in the case of positional obstruction to superficial blood flow in the saphenous networks (stretching and compression by crossing the legs). The most important of these perforating veins are Boyd’s perforators and Cockett’s perforators. In contrast, in the case of hypertension in the deep venous network, their short, direct course facilitates the development of skin lesions at this level.
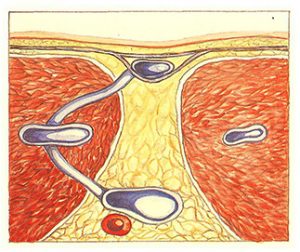
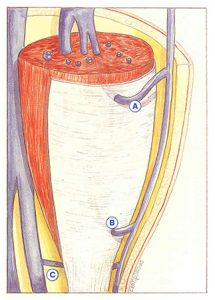
The main perforating veins connected to intramuscular veins are the medial gastrocnemius perforating veins. They are usually multibranched (Figure 99), and receive fine collaterals derived from the muscle. By draining their own muscle territory, they act as an intermediary for the calf muscle pump to act on the saphenous networks and intersaphenous arches. According to Gillot, a gastrocnemius perforating vein is not only a branch of the recipient gastrocnemius vein, but its initial segment is also an integral part of this gastrocnemius vein.
When the intramuscular venous network is the site of hypertension (dilatation or incompetence of gastrocnemius veins, insufficient muscle pump, obstruction to blood flow), transgastrocnemius intersaphenous connections can ensure diffusion of reflux to saphenous trunks, intersaphenous arches, and/or collaterals.
The rich network of medial gastrocnemius perforating veins, in combination with intersaphenous arches, transforms the middle segment of the short saphenous vein into a real exchange center between the long and short saphenous veins and medial gastrocnemius veins.
The short saphenous vein is also usually suprafascial in this zone, which explains why, in contrast with the long saphenous vein, the short saphenous vein can present a greater caliber than its junction with the deep system. Ultrasound investigation of the trunk must therefore be just as detailed as that of the saphenopopliteal junction and proximal reflux. Precise mapping of intersaphenous arches and gastrocnemius perforating veins is absolutely essential. The absence of these data can account for certain failures of isolated saphenopopliteal junction ligation.
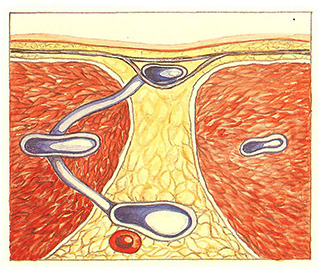
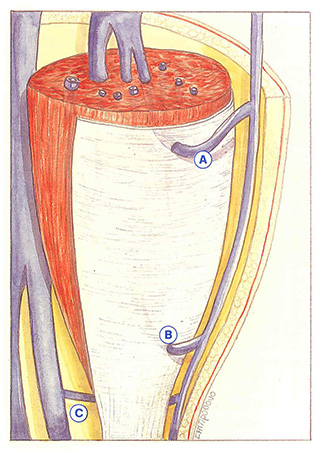
Finally, two portions of intramuscular perforating veins can be distinguished (Figure 100)
- the first, subfascial, portion is the longer of the two. It has a descending course until it crosses the fascia, where it describes a concave upwards curvature;
- the second, suprafascial, portion ascends over a much shorter distance;
These perforating veins possess two or three valves situated at their origin and in the zone of their transfascial passage.
Further reading
Dortu J., Dortu JA. Les veines perforantes du membre inférieur : physiologie et physiopathologie. Phlébologie, 1994; 47: 167-75.
Gillot C. Les veines perforantes inférieures de la jambe, de la cheville et du pied. Phlébologie, 1994; 47: 76-104.
Thomson H. The surgical anatomy of the superficial and perforating veins of the lower limb. Annals of the Royal College of Surgeons, 1979; 61: 197-205.