Hemodynamic aspects
The popliteal fossa, a real venous crossroads, is the site of anastomosis of three superimposed venous planes: the short saphenous vein and its collaterals, which drain the subcutaneous zone: the medial and lateral gastrocnemius veins, which drain the intramuscular zone: and, finally, the popliteal vein, sometimes duplicated by a collateral vessel, which drains blood from the intermuscular zone (from peroneal, anterior tibial, and posterior tibial veins).
From a functional point of view, under physiological conditions, the intramuscular gastrocnemius veins represent a venous reservoir at the center of the “peripheral heart,” corresponding to the calf muscle pump. During muscle contraction, blood is expelled at a very high flow rate to the popliteal vein. During muscle relaxation, or in the case of sudden pressure variations in the popliteal vein (for example. breath-holding effort), the extramuscular portion of the gastrocnemius veins, which travels in the loose connective tissue of the popliteal fossa, dilates and absorbs these pressure rises.
When the gastrocnemius veins are abnormally dilated (Figure 75A), ), they form a larger blood reservoir. In the case of sudden muscle contraction associated with breath-holding effort, the blood from intramuscular gastrocnemius veins is ejected at a high flow rate into the popliteal network (Figure 75B). Deep venous hypertension (breath-holding effort, obstacle to evacuation of blood by the deep venous network) impairs drainage, resulting in a marked rise in popliteal venous pressure. In this example, the short saphenous vein represents an important pathway of evacuation of excess blood in the gastrocnemius veins and therefore constitutes a second “shock absorber”.

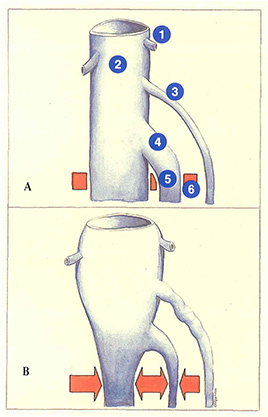
Ligation of the saphenopopliteal junction associated with stripping will therefore eliminate this excess pressure shock-absorbing mechanism and facilitate the rapid development of a perforating vessel in the popliteal fossa.
These features can lead to two conclusions:
- marked ectasia of the medial gastrocnemius veins can compromise the results of short
saphenous vein surgery by predisposing to early recurrence via a perforator in the popliteal fossa; - ligation of the common trunk of the gastrocnemius veins has no consequence in the case of a lambda termination or when the medial gastrocnemius venous network can drain by another route into the popliteal network. In contrast, in the absence of such a drainage, this ligation will induce hypertension in the intramuscular network during contraction, which causes reflux into the gastrocnemius perforators. Several authors have therefore advised against ligation of the common trunk of the gastrocnemius veins in the popliteal fossa.
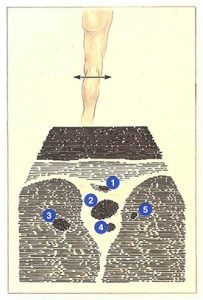
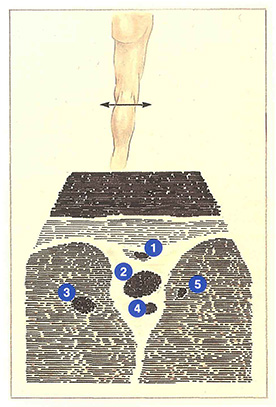
The veins of the popliteal fossa have a characteristic placement on the ultrasound screen (Figure 76),The popliteal vein, lying between the muscles and above the popliteal artery, has the largest caliber. In 20% of cases, the popliteal vein is duplicated by a collateral venous channel. Although it has the same diameter as the popliteal artery, it can be distinguished by the fact that it can be compressed by the ultrasound transducer.
Above the popliteal vein. the short saphenous vein travels in a fascial sheath. The gastrocnemius veins appear in the muscles surrounding the popliteal vein.
Further reading
Daniel C. Le syndrome des veines jumelles. Actualité Vasculaire Internationale, 1992; 6 : 16-22.
Gillot C. La perforante polaire inférieure du muscle jumeau interne. Phlébologie, Édition Médicale Média Internationale, Congrès de Bruxelles, vol 1, 1983.
Thierry L. Physiology of the muscular veins. Phlébologie, Éditions John Libbey Eurotext, Montréal 1992.
Van der Stricht J. Staelens I. Les veines musculaires du mollet. Phlébologie 1994; 47, 2: 135-43.