Perineal varices
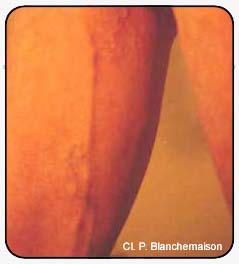
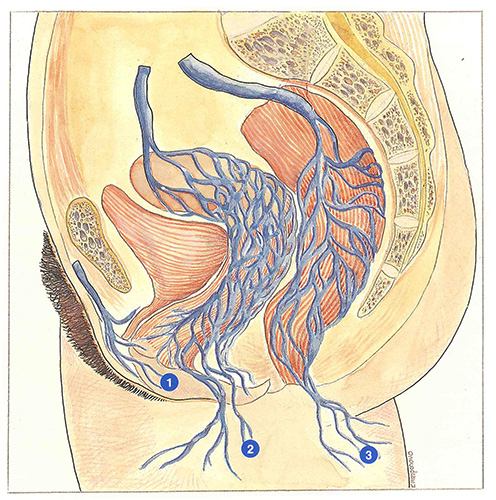
These varicose veins, frequent in women after pregnancies, are more rarely observed in men, apart from competitive sportsmen (Figure 35). They are situated very superficially medial to the long saphenous vein and tend to be multiple, anastomosed between each other and tortuous. They communicate directly with the intrapelvic venous network via the internal pudendal veins or via uterine veins in women. They generally respond well to sclerosis or phlebectomy.
When they are the site of reflux, they can supply the long saphenous trunk, with a persistently competent arch, or a varicose system of the leg independent of the long saphenous vein.
After stripping, in the absence of any recurrence at the saphenofemoral junction, they are often responsible for persistence or recurrence of varicose veins.
As their intrapelvic communications are inaccessible to treatment, they always retain a potential for subsequent development. Consequently, the perineal region must be carefully monitored, especially during subsequent pregnancies.

Further reading
Varices périnéales
Bergan J.J., Yao J. Venous disorders, W.B. Saunders Company, 1991.
Varices vulvaires
Dixon J.A., Mitchell W.A. Venographic and surgical observations in vulval varicose veins. Surg Gynecol Obst, 1970, 131
458-64.
Lechter A., Alvarey A., Lopez G. Pelvic varices and gonadal
veins. Phlebolo , 1989, 2: 181-8.
Varices fessières
Lefebvre D., Bastide G., Vaysse Ph., Roux R., Joly R. Connexions veineuses intra et extrapelviennes. Étude anatomique. Phlébologie, 1989, 42: 385-9.
Van Der Stricht J., Van Oppens C. Where do vulvar varices come from ? Phlébologie 89, J. Libbey Eurotext, 1989 473-5.