Ultrasonographic anatomy
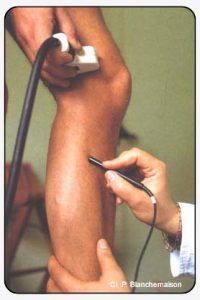
One of the major advances in phlebology certainly consists of investigation of superficial veins by ultrasonography linked to Doppler. Morphological and anatomical data are also obtained with an increasingly better resolution. Doppler ultrasound, which assesses the velocity of displacement of red blood cells, identifies the direction of circulation of venous blood and therefore allows a dynamic investigation (Figure 5).
Equipment
Investigation of superficial veins by ultrasonography uses three types of apparatus.
- Two-dimensional (2D) ultrasonography provides a direct, real-time image of the vein (Figure 6). It allows a morphological study: origin of reflux, diameter of venous trunks, parietal thickness, presence of thrombosis (direct visualization, incompressibility). It must always be combined with continuous Doppler.
- Ultrasonography and pulsed Doppler, combined in the same transducer, allow positioning of a target visualized on the screen. Reflux can therefore be detected by an audio signal in certain difficult zones in which the veins are sometimes superimposed: varicose veins of the popliteal fossa, the medial gastrocnemial veins, tributaries of the saphenofemoral junction.
- Color ultrasonography is also linked to pulsed Doppler. In this case, a visual image is added to the audio signal: the direction of blood flow is shown as red towards the feet and blue towards the heart (Figure7).However, apart from the investigation of deep venous incompetence, color Doppler ultrasonography does not appear to be superior to simple pulsed Doppler ultrasound.
In addition to the type of apparatus used, two other parameters also determine the choice of equipment: the frequency and the type of transducer.

Superimposition of the superficial femoral vein and artery, with origin of an incompetent accessory saphenous vein.
The choice of frequency is based on the depth of the vein to be examined. The higher the frequency, the better the image of superficial anatomical structures. However, this choice remains a compromise between lateral resolution, depth of field and focal distance. In practice, a 3.5 MHz transducer is used for intrapelvic veins, a 7.5 MHz transducer is used for intramuscular and saphenous veins, a 13 MHz transducer is used for the infrapapillary venous network and, more recently, a 20 MHz transducer is used for the intradermal system.
Two types of transducer are available: sectorial or linear. Linear transducers limit the size of the acoustic shadow compared to sectorial transducers, which is a useful feature in venous disease. However, sectorial transducers, which are smaller and easier to operate, have been preferred for a long time to linear transducers, which are considered to be too bulky. Small linear transducers have been recently introduced, which considerably improve the investigation of superficial veins.
Ultrasonographic appearance of veins of the lower limbs
Ultrasonography provides a large amount of anatomical information.
- Diameter of the veins
The frequency of the transducer determines the lateral resolution and, consequently, the smallest detectable diameter. Veins of the lower limbs are generally studied with a 7.5 MHz transducer, which, at best, allows visualization of veins 2 mm in diameter (for example, tributaries of the arch of the long saphenous vein, but also certain perforators). In contrast, a 20 MHz transducer can detect veins 0.3 mm in diameter (intradermal veins).
Classically, the long saphenous vein measures 3 to 5 mm in diameter. This diameter can increase physiologically by 1 to 3 mm: hyperthermia, prolonged standing, pelvic hypertension (induced by the Valsalva manoeuvre), pregnancy, or menstrual period:
- Patency
In the absence of thrombus, the venous lumen is an echo-free and totally compressible structure.
When red blood cells agglutinate into rouleaux, the circulating blood becomes echogenic. This phenomenon is observed in venous junctions (for example, the saphenofemoral junction), adjacent to valves, but also in the presence of venous stasis or during pregnancy, in which 2D ultrasonography provides hemodynamic data.
- Valves
Valves are visualized either directly in the form of an echogenic line forming a flap in the venous lumen, or indirectly, outlined by the echogenicity of the perivalvular blood.
- Thickness of the venous wall
Under basal conditions, the venous wall is seen as a fine, flexible, poorly echogenic, and well defined line, in the absence of dynamic blurring. Parietal thickening is observed in prevaricose saphenous veins in children, and in old, nonvaricose veins in the elderly, but also in toplevel athletes or even in veins “arterialized” by saphenous vein bypass grafts.
Once an anatomo-ultrasonographic correlation has been perfectly defined, various applications could be envisaged: assessment of the qualities of a saphenous vein prior to bypass grafts, evaluation of the effects of treatment on parietal thickness, search for criteria allowing the application of conservative treatments.
- Detection of perforating veins
Ultrasonography precisely locates the origin, course and termination of perforating veins and any of their supra and subaponeurotic tributaries. Consequently, only ultrasonography has allowed visualization of perforating veins with a vertical and ascending intramuscular course, while varicography is unable to opacify such vessels. Precise location of perforating veins, associated with identification of the sites of venous reflux, has led to the concept of hemodynamic mapping of superficial veins.
Further reading
Blanchemaison Ph., Chahine D., Mouren X., Caillard Ph. La cartographie veineuse superficielle par échographie Doppler. In Phlébologie 92, J. Libbey Eurotext, Paris, 1992.
Franceschi C., Franco G., Luizy P., Tanitte M. Précis d’échotomographie vasculaire. Vigot, Paris, 1992.
Laroche JR, Muller G. Atlas d’écho-Doppler pulsé veineux. Laboratoires Servier Ed, Orléans, 1991.