Duplicated junction
Duplication of the arch of the long saphenous vein is so rare that it is only mentioned in a few publications concerning anatomical variants of the saphenofemoral junction. Two elements differentiate this variant from the classical configuration of an accessory saphenous vein associated with the main long saphenous trunk:
– the two long saphenous veins have the same caliber and drain a common cutaneous territory;
– they both lie in the same plane, parallel to the skin and run along the muscular aponeurosis.

The duplicated saphenous veins therefore differ from accessory saphenous veins which have a smaller caliber and, more importantly, ensure the drainage of different cutaneous territories.
These accessory saphenous veins can generate post-stripping varicosities. (Click here)
Duplication of the long saphenous vein is confused with tributaries, which may appear, on Doppler ultrasound, as a large-diameter superficial duplication, as the real long saphenous trunk, with a small diameter and sometimes poorly demonstrated on ultrasonography, travels along the aponeurosis.
Thus; during stripping, there is a risk that the stripper may enter the large-caliber superficial duplication, leaving the hypoplastic saphenous trunk in place.
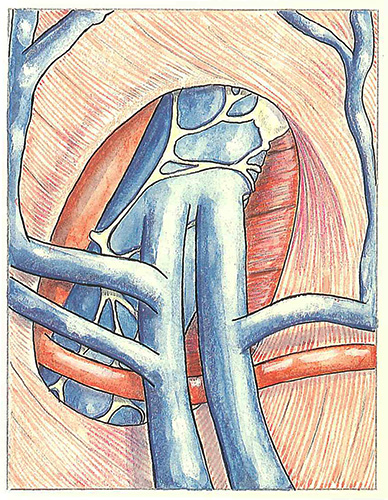
Schematically, three types of duplicated saphenous arch can be described:
- A common junction
above the duplication (Figure 16)
This constitutes a real trap when the duplication is situated outside the surgeon’s field of vision;
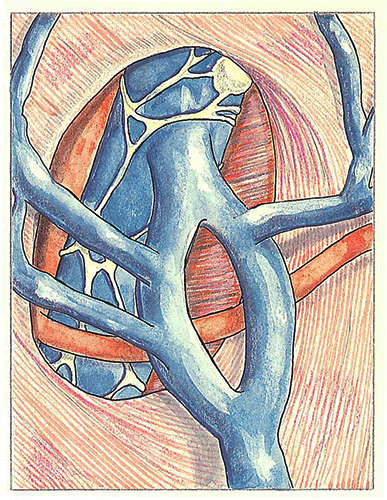
- Two separate junctions (Figure 17)
The two long saphenous veins enter the femoral vein separately and each one receives its own tributaries;
- A common junction
and an insular duplication (Figure 18)
This variant also constitutes a surgical trap inasmuch as the duplication is poorly accessible to the surgeon’s field of vision. In this case, recurrences may arise from the duplication left in place, especially when it is centered around a perforating vein. The approach to such variants is preventive and consists of performing preoperative mapping of the superficial veins.
Further reading
Davy A. Notions d’anatomie veineuse en phlébologie quotidienne. Phlébologie en pratique quotidienne. Expansion scientifique, Paris, 1982.
Mozzon L., Venier E., Gonano N., Biasi G. Sur un cas de double crosse saphénienne. Phlébologie 89, A. Davy, R. Stemmer Eds, 1989, J. Libbey Eurotext Ltd, 14-15.