Knee and leg
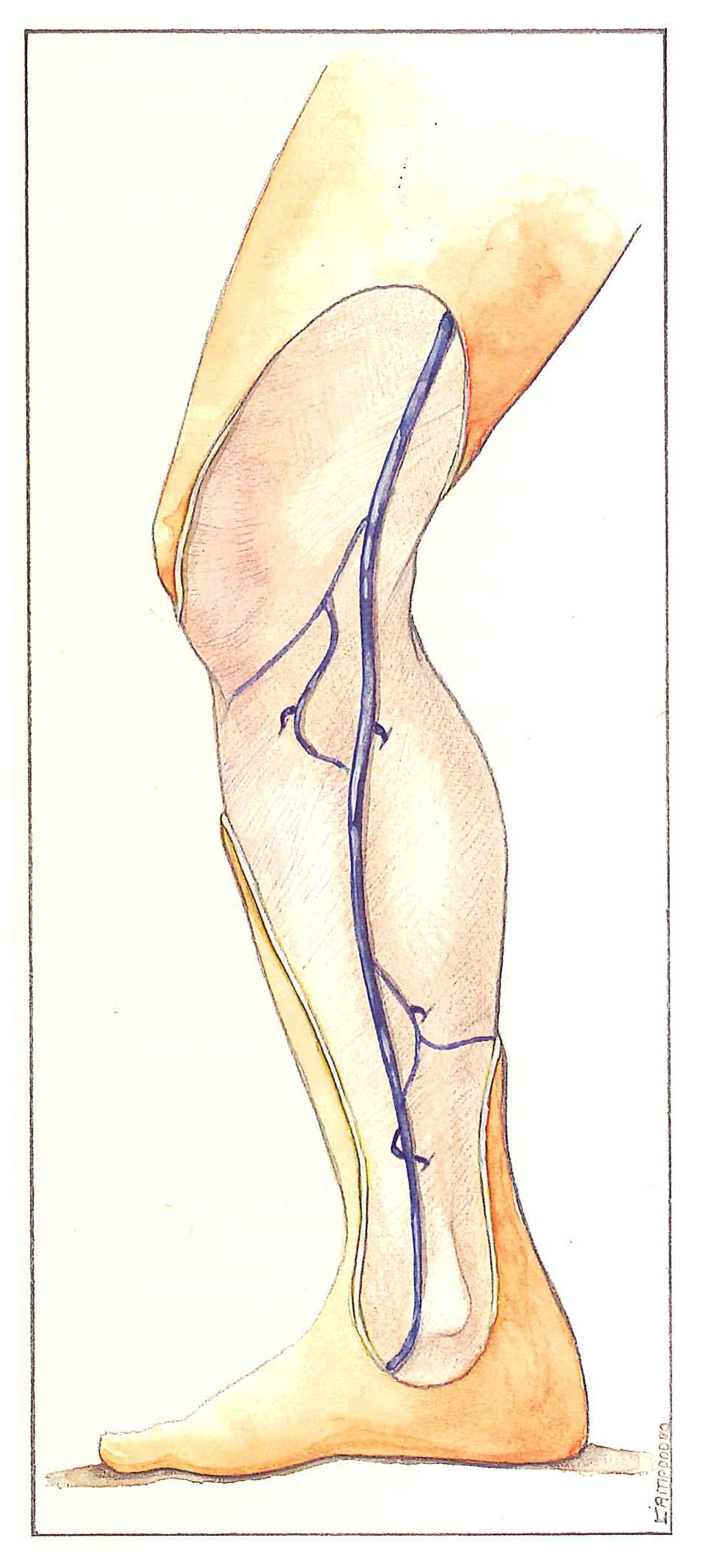
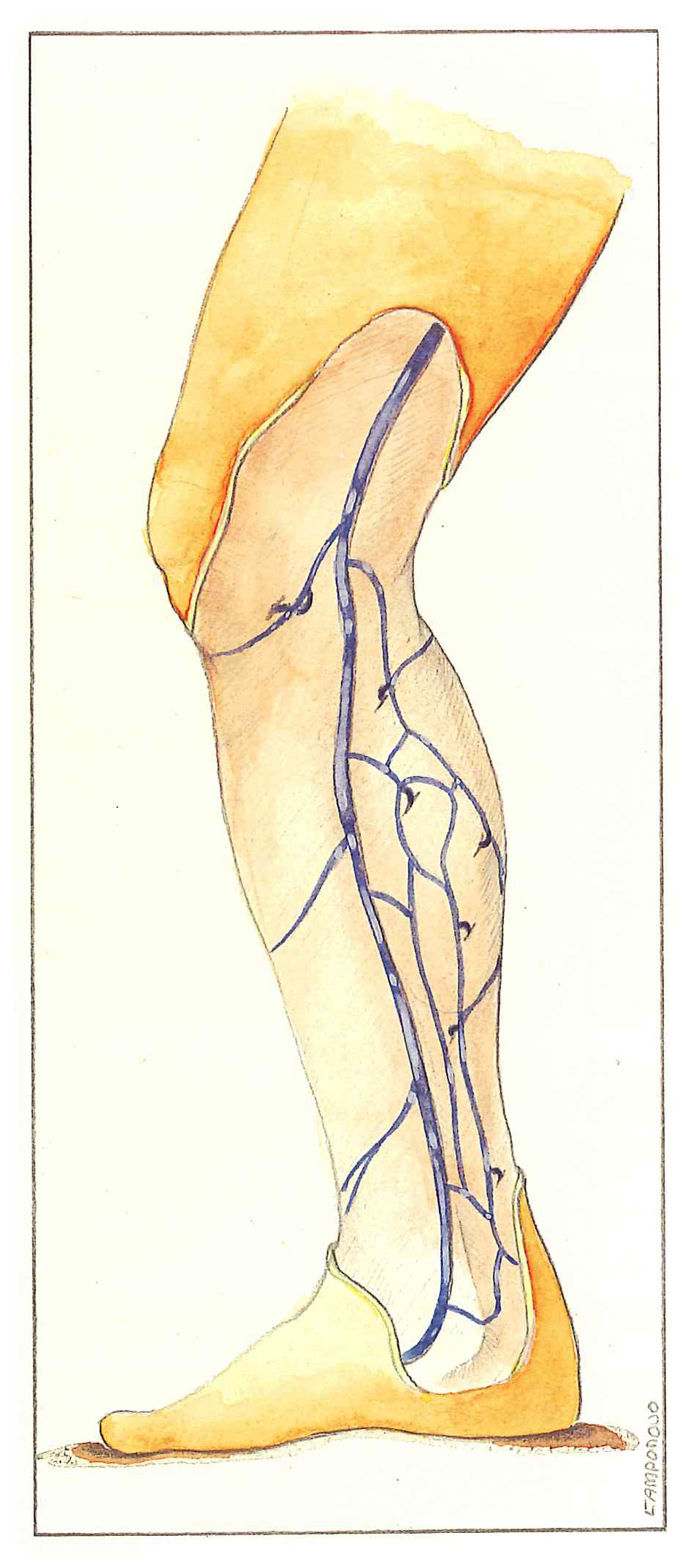
Transverse sections are necessary in the thigh because of the superimposition of superficial veins. This problem no longer applies in the leg, as the subcutaneous tissues are thinner. On the other hand, the various networks form complex anastomoses and hemodynamic circuits in a single plane. The surface anatomy of these veins can therefore be easily studied with the patient standing.
Perforating veins of the knee and leg are presumed to be involved in the pathogenesis of varicose veins to such a point that some authors have recommended systematic eradication of these veins in order to prevent recurrence.
These perforating veins were initially classified according to their level: lower third of the leg for low Cockett’s perforators, middle third for medial gastrocnemius perforating veins and high Cockett’s perforators, and finally, the upper third of the leg for Boyd’s perforators.
The first authors to systematically describe these vessels attributed fairly constant anatomical sites, aligned along an imaginary vertical line, called Linton’s line. This line is parallel to the long saphenous vein in the leg and lies one fingerbreadth behind the medial malleolus.
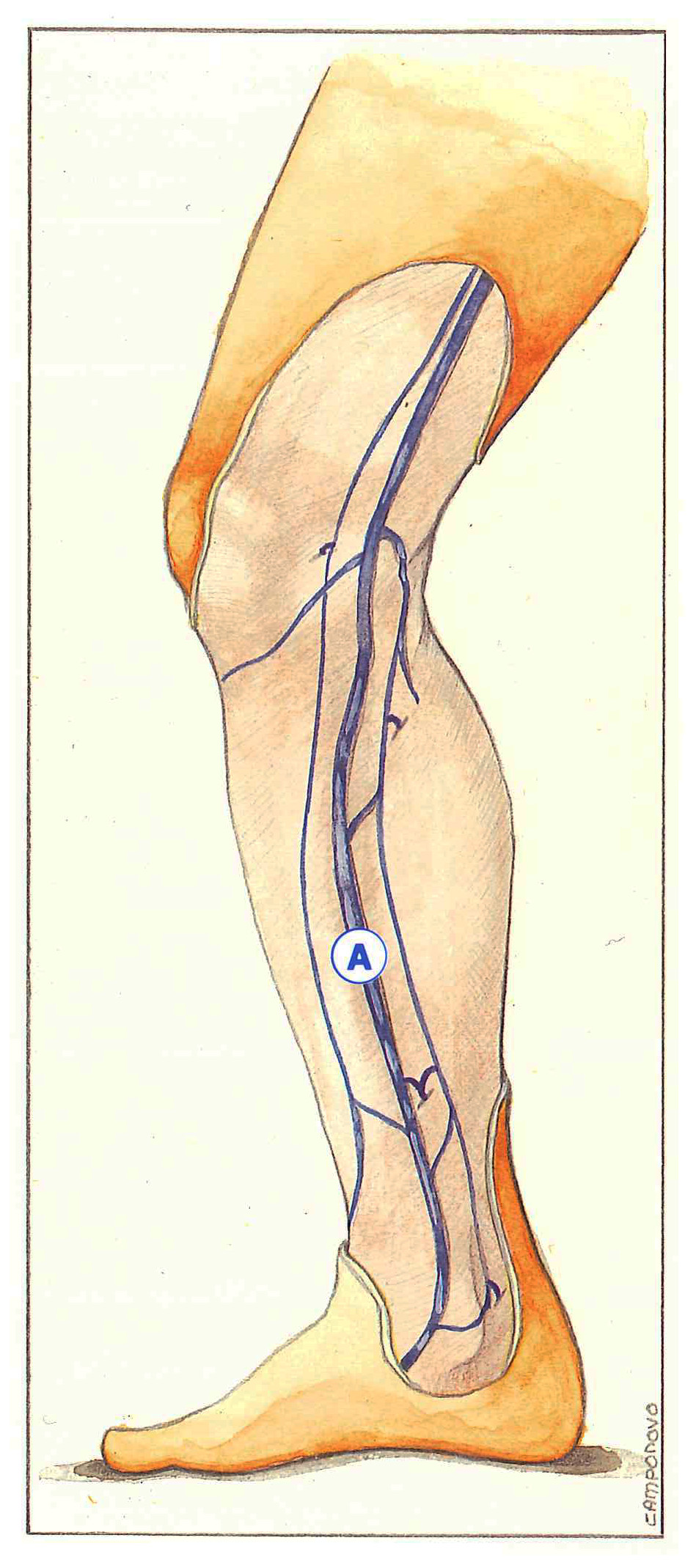
From below upwards, the various perforating veins correspond to Cockett I (precisely 67 cm from the ground), Cockett II (13.5 cm), Cockett III (18.5 cm), and then the so-called “24-cm” perforators. These veins communicate between the posterior branch of the long saphenous vein in the leg (Leonardo’s vein) and the posterior tibial veins.
This constant site “perforator rule” is contested by other anatomists. Some believe that the majority of perforating veins of this region are located on collateral vessels connecting the long saphenous vein to its posterior branch, while others consider that they are situated randomly with a particularly variable distance from the ground.
From an anatomical and functional point of view, these perforating veins can be classified not according to their level of anastomosis, but according to their position in relation to the saphenous vein. The type of circuit in which they participate can be more clearly explained on venous mapping.
We therefore propose to distinguish four types of perforating veins in the knee and leg:

The types of venovenous shunts observed can be defined by simultaneously taking into account the anatomical situation of these perforating veins and the hemodynamic circuit in which they participate.
Most of these perforating veins are globally attracted towards the long saphenous. vein. They can nevertheless form complex, independent hemodynamic circuits. Some of them are incompetent during muscular systole and diastole, while others are only incompetent during diastole (click here). Other circuits allow reentry of an overlying reflux. They are also sometimes connected to each other by longitudinal interperforator anastomoses responsible for recurrences.
The perforating veins of this region communicate with various deep veins. Perforating veins of the medial region below the knee (Boyd’s perforators) open into posterior tibial veins or the tibioperoneal trunk. Variable numbers (3 to 6) of usually indirect perforators are grouped together and arise from an accessory saphenous vein or tributary. These small-caliber vessels describe a long intramuscular course and are only rarely responsible for massive reflux and are usually responsible for varicosities of the medial regions of the knees.
Very rarely, a great anastomotic vein can arise in the region of Boyd’s perforators. It remains a tributary to the cutaneous branch of the anastomotic artery with which it perforates the aponeurosis of the adductor canal. Draining into the femoral vein, but only emerging from the aponeurosis medially below the knee, this vein actually represents a variant of an adductor canal perforating vein. It connects the femoral vein with the saphenous vein in the leg or with the accessory saphenous vein or tributaries.
Muscular perforating veins of the medial surface of the calf anastomose with medial gastrocnemius veins. C. Gillot subdivides them according to their site of muscular penetration into upper, middle, and lower pole veins. Only the latter anastomose with the short saphenous vein. These medial gastrocnemius perforating veins, generally indirect, with multiple branches and receiving intramuscular branches, arise from a diversion of the long saphenous trunk (Figure 62), an accessory saphenous vein (Figure 63), the calf plexus (Figure 64), or an intersaphenous communication (Figure 65). These medial gastrocnemius perforators are common and are involved in recurrences and extension «of superficial thromboses towards deep veins.
All of the so-called Cockett’s perforators anastomose with posterior tibial veins. They may arise from Leonardo da Vinci’s vein, but also from communications between this vein and the saphenous vein, a posterior accessory saphenous vein, or tributaries. The more proximal veins often act as reentries for an overlying reflux. The most serious vessels from a pathogenic point of view are low Cockett perforators, situated one handsbreadth above the medial malleolus with a short and direct course. Ectatic Cockett perforators are difficult to access, but are palpable well below the site of aponeurotic perforation, in a zone of cellulitis which they generate or accentuate.
Perforating veins of the anterolateral region of the leg anastomose with peroneal or anterior tibial veins. They are generally reentry perforating veins for reflux derived from the anterior saphenous network of the thigh. They can generate varicosities, but are only exceptionally responsible for trophic disorders. All these perforating veins, together with tributaries and accessory saphenous veins, constitute a veritable long saphenous system. Any blood reflux will be part of an original circuit, a venovenous shunt involving dilated perforating veins which are either incompetent or reentry pathways towards the deep veins.
Further reading
Dodd H., Cockett EB. The pathology and surgery of the veins of the lower limb. Londres, Churchill Livingstone, 1976.
Fischer R., Fulleman N.H., Alder W. A propos d’un dogme phlébologique sur les localisations des perforantes de Cockett. Phlébologie 1992; 45: 207-12.
Gillot C. Anatomie chirurgicale des perforantes de la jambe. Phlébologie 1987; 40: 563-74.
Staubesand J., Stemmer R. Études anatomiques sur la constance des perforantes de Cockett. Phlébologie 1987; 40: 599-604.