Ectatic junction
According to recognized anatomical constants, the saphenofemoral junction or arch of the long saphenous vein is situated four cm below the inguinal ligament.
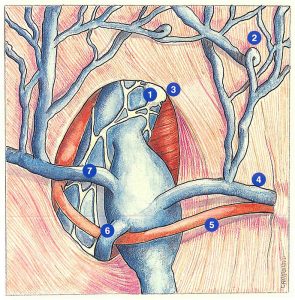
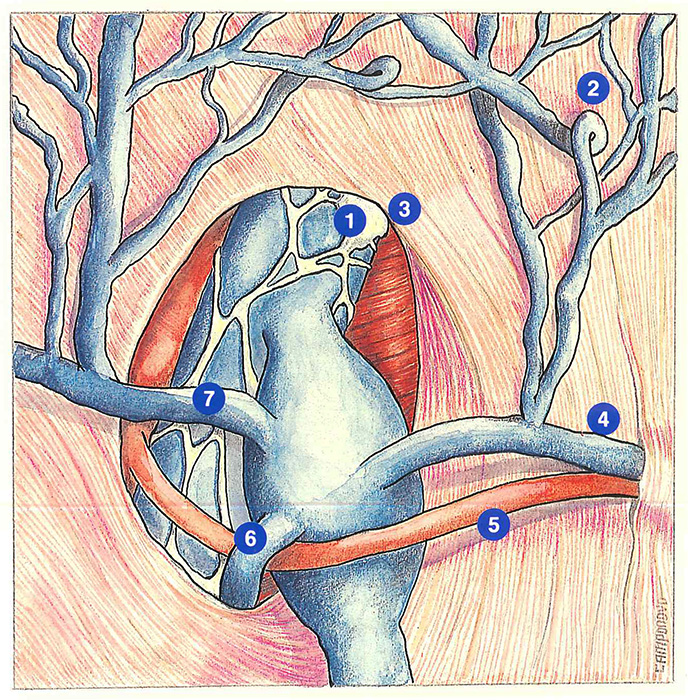
The saphenous opening, delimited by Allan Burns’ falciform ligament, contains, from medial to lateral: the internal inguinal lymph nodes, the femoral vein which receives the arch of the long saphenous vein, and the common. femoral artery.
According to Lanz and Wachsmuth, in 37 of cases, the saphenous vein forms a “venous star” composed of:
one or several external pudendal veins,
the epigastric vein or abdominal subcutaneous vein,
the superficial circumflex iliac vein,
one or several accessory saphenous veins.
Note that the internal pudendal artery passes anteriorly or posteriorly to the arch of the long saphenous vein in the saphenofemoral angle.
We will consider three types of ectasia of the saphenofemoral junction. In the first type, which can be described as “ideal” and also the most classically described (Figure 13), the position of the ectasia allows resection of the saphenofemoral junction associated with ligation as close as possible to the femoral vein. Application of two opposing clips or isolated resection of the saphenofemoral junction can also be performed.
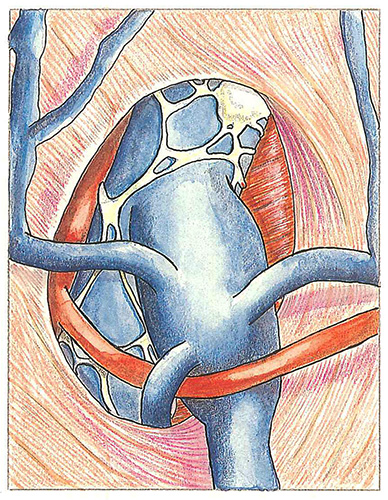
When the saphenofemoral junction is surrounded by the ectasia (Figure 14), only resection of the saphenofemoral junction with femoral arterioplasty can be performed. In this case, isolated ligation of the junction or the use of clips is very difficult, or even impossible.
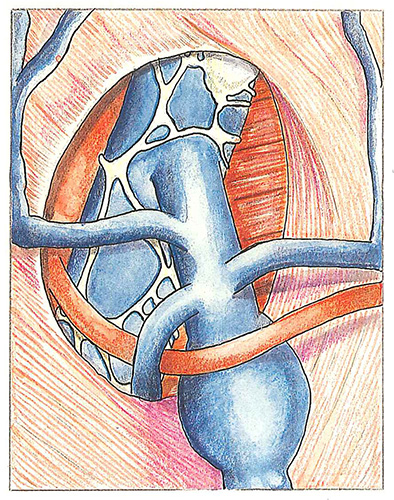
The third type of ectasia (Figure 15) constitutes a real trap: the ectasia no longer involves the saphenofemoral junction, but the underlying saphenous trunk. This ectasia may be associated with reflux by an internai pudendal tributary, communicating with a uterine vein. Extensive resection of the saphenofemoral junc tion with stripping of the saphenous trunk appears to be the most appropriate strategy in this case.
Further reading
Von Lantz T, Wachsmuth W. Praktische Anatomie, Springer, Berlin, 1959, I.
Minnes S, Depreux R. Variations anatomiques des affluents de la crosse de la veine saphène interne. C.R. Assoc. Anat., 1970, 55: 459-67.
Furderer C, Marescaux l, Stemmer R. Les crosses saphéniennes. Anatomie et concepts thérapeutiques. Phlébologie, 1986, 39 (1) : 9-14.