Termination and associated reflux
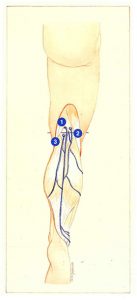
In the popliteal fossa, the short saphenous vein curves 4 cm above the popliteal crease to describe an anterior concave arch before terminating on the posterior or posterolateral surface of the popliteal vein (Figure 77).
However, there are many variants of this classical arrangement, and several classifications of the modes of termination of the short saphenous vein have been proposed on the basis of surgical and radiographic arguments.
Mercier’s classification describes six types of terminations:
I: The saphenopopliteal junction is situated 2 to 15 cm above the popliteal crease; this situation is observed in half of all cases;
II: The saphenopopliteal junction is also situated 2 to 15 cm above the popliteal crease, but is prolonged by a trunk which anastomoses with the long saphenous vein;
III: The so-called high saphenopopliteal junction terminates on the posterior aspect of the thigh, in the femoral vein, which communicates with the long saphenous vein;

IV: The saphenopopliteal junction does not exist. and the short saphenous vein terminates exclusively in the long saphenous vein;
V: The high saphenopopliteal junction terminates on the posterior aspect of the thigh, in the femoral vein;
VI: The saphenopopliteal junction is complex, with a number of intramuscular anastomoses.
Based on the analysis of 120 dissections. Kosinsky has also described direct termination of the short saphenous vein in the popliteal vein in 57% of cases and into the gastrocneemius veins in 10% of cases.
Based on similar criteria, Haeger reported that the termination of the short saphenous vein was frequently (6000 of cases) situated 3 cm above the popliteal crease, but situated below this crease in only 8% of cases.
In contrast, based on radiographic data, May and Nissl reported that 76% of terminations were situated in the 3 cm overlapping the popliteal crease. According to these authors, the termination is situated below the popliteal crease in only 1.5% of individuals.
For practical purposes, we propose a classification which simultaneously takes into account the modes of termination of the short saphenous vein and the sources of associated reflux. which are frequently involved in posttreatment recurrence. In parallel, it seems essential to describe saphenopopliteal junctions with an atypical morphology, independently of their situation, which interfere with saphenopopliteal junction ligation flush with the popliteal vein.
Such a classification is based on ultrasound and surgical criteria, and can be used as a basis to define the following therapeutic indications:
Type I
The saphenopopliteal junction is situated in a classical anatomical position (in the popliteal fossa. usually 3 or 4 cm above the popliteal crease):
- without any other associated source of reflux:
- with associated reflux in the popliteal fossa via a perforating vein of the popliteal fossa or a gastrocnemius perforating vein (Figure 77);
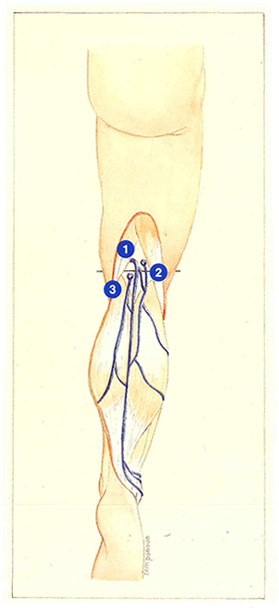
- with associated reflux from the thigh derived from a trunk of the long saphenous vein (Giacomini’s vein) or a perinea) vein, via a gluteal or profunda femoris perforating vein or, finally, via an anterior branch of the long saphenous vein (Figure 78);
- atypical morphology of the saphenopopliteal junction (Figure 79).
Type II
The saphenopopliteal junction has a high position, more than 5 cm above the popliteal crease:
- without any other source of associated reflux;
- with associated reflux from the thigh derived from a trunk of the long saphenous vein (Giacomini’s vein) or a perineal vein, via a gluteal or profunda femoris perforating vein or via an anterior branch of the long saphenous vein.
Type III
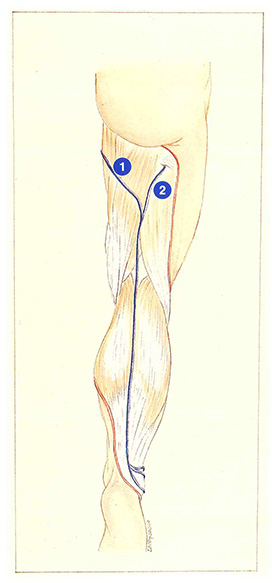
The saphenopopliteal junction does not exist (Figure 81);
- the short saphenous vein terminates directly in the long saphenous vein;
- the short saphenous vein terminates in the profunda femoris vein at the top of the thigh.
Atypical morphology of the saphenopopliteal junction
An understanding of the morphological variants of the saphenopopliteal junction is essential in order to define the optimal surgical indications.
Short saphenous vein and popliteal fossa reflux surgery must achieve certain objectives:
- elimination of only incompetent venous trunks (reflux can be observed from perforating veins of the popliteal fossa without any concomitant lesion of the short saphenous vein);
- elimination of all sources of reflux (the many sources of reflux associated with the short saphenous vein must be clearly defined);
- saphenopopliteal junction ligation, flush with the popliteal vein.
This last procedure may be difficult to perform in the case of atypical morphology of the saphenopopliteal junction.
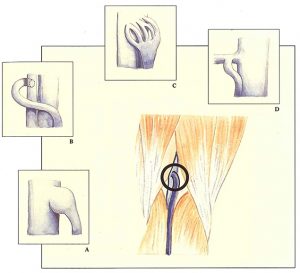
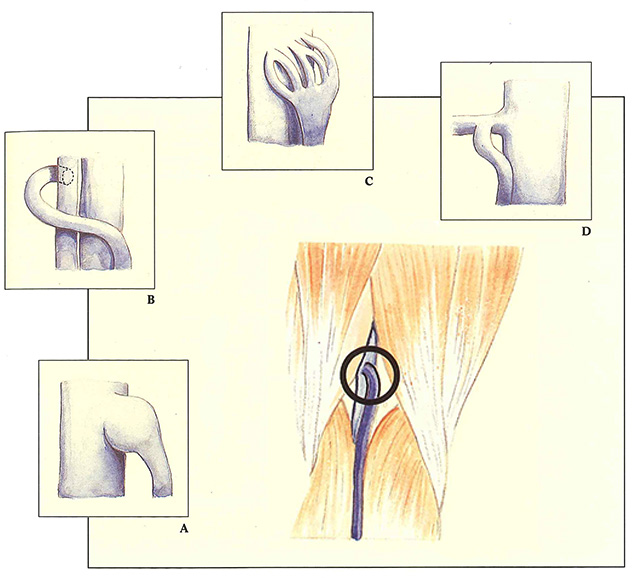
Ideally. the short saphenous vein terminates on the posterior or posterolateral surface of the popliteal vein (Figure 77), but four other modes of termination may be observed:
- after curving deeply, the short saphenous vein describes an arch and presents a subfascial aneurysmal dilatation, at the site of its junction with the popliteal vein (Figure 79A);
- the short saphenous vein turns around the popliteal vein medially and then describes a second, laterally concave curvature before terminating anteriorly in a duplication of the popliteal vein (Figure 79B);
- the saphenopopliteal junction has a delta termination in the popliteal vein, sometimes anastomosing with the common trunk of the medial or lateral gastrocnemius veins (Figure 79C);
- the short saphenous vein terminates in a collateral of the popliteal vein (Figure 79D).
All of these situations can constitute an obstacle to a saphenopopliteal junction ligation flush with the popliteal vein. Phlebographic studies by Garcia Marquès have clearly demonstrated that incomplete resection of the saphenopopliteal junction can be responsible for recurrence from the short saphenous stump. These data should convince us of the necessity for extensive surgery comprising wide, and therefore, traumatic dissection. carrying the risk of unsightly scars. Short-term recurrences in the popliteal fossa have been observed despite a procedure having been performed by an experienced surgeon and, inversely, saphenopopliteal junction ligations performed away from the popliteal vein do not systematically give rise to recurrences.
In fact, it is not sufficient to take only the anatomical parameters into account. The popliteal fossa is a highly mobile zone of confluence which is subject to very marked pressure variations. The hemodynamic parameters therefore represent an essential element. Recurrence on a short saphenous stump may therefore occur when it is subject to high pressures from the popliteal or medial gastrocnemius networks.
Therapeutic decisions must therefore be based on a combination of anatomical and hemodynamic criteria, in addition to evaluation of the clinical context, risk factors, and condition of the skin. This is the only way to ensure the best compromise between efficacy and an esthetic result.
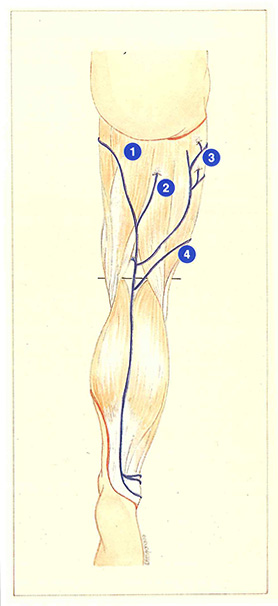
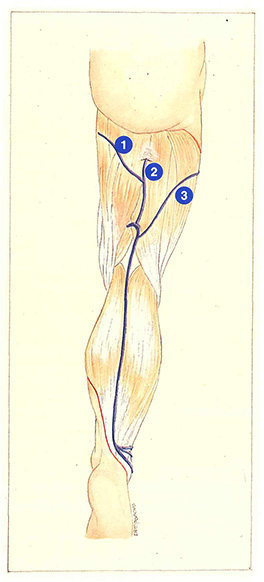
A high saphenopopliteal junction represents another source of operative difficulty (Figure 80). When the junction is situated above the popliteal fossa, it is frequently deep and generally requires a large incision, with the risk of a frequently unsightly scar. especially as it lies outside the popliteal crease.

The saphenopopliteal junction is often identified in an atypical position by duplex ultrasound, lying above the real junction. In fact, this detection is performed in the standing position and the junction is then subject to traction effects exerted by the fascia of hamstring muscles and therefore ascends slightly. This traction disappears in the ventral supine position.
Reflux associated with a high short saphenous vein can be derived from:
- the long saphenous vein via a Giacomini communicating vein. It should be noted that, in the case of postural or postthrombotic obstacle to drainage of the popliteal vein, ascending reflux can develop during muscle contraction. from the saphenopopliteal junction towards Giacomini’s vein and the long saphenous vein. This situation can lead to inappropriate long saphenous vein stripping, responsible for reflux in the popliteal fossa;
- a perineal venous network;
- a gluteal or profunda femoris perforating vein with an ascending. intramuscular course;
- anterior branch of the long saphenous vein.
In 15% to 20% of cases, the saphenopopliteal junction is nonexistent (Figure 81). The short saphenous vein continues along the posterior surface of the thigh. then curves medially to terminate in the Tong saphenous vein, or more deeply in the profunda femoris vein. In this last case, the intramuscular course of the short saphenous vein prevents complete surgery. However, a solution can be provided by introducing a catheter or an endoscope into the popliteal crease, which is then advanced as far as the proximal part of the thigh.

Further reading
Daniel C. Le syndrome des veines jumelles. Actualité Vasculaire Internationale, 1992; 6 : 16-22.
Gillot C. La perforante polaire inférieure du muscle jumeau interne. Phlébologie, Édition Médicale Média Internationale, Congrès de Bruxelles, vol 1, 1983.
Thierry L. Physiology of the muscular veins. Phlébologie, Éditions John Libbey Eurotext, Montréal 1992.
Van der Stricht J. Staelens I. Les veines musculaires du mollet. Phlébologie 1994; 47, 2: 135-43.