Anatomy of recurrences following resection of the saphenofemoral junction
Mechanisms
True recurrences must be distinguished from residual varicose veins. There are two main causes for recurrence following groin surgery:
– anatomical causes
– hemodynamic causes
- anatomical causes are situated either at or away from the saphenofemoral junction (Figure 41).
In the first case, they can result from a technical error:
– excessively low ligation of the long saphenous vein away from the saphenofemoral junction, with persistence of a stump of arch (6),
– persistence of a subfascial anterior branch (the commonest cause) (3) ,
– presence of an accessory saphenous vein (7)
– presence of a tributary draining directly into the femoral vein (2).
Lastly, recurrences secondary to an anatomical cause at the junction are sometimes due to an error of strategy: isolated ligation, clipping, distal leaks, etc.
Anatomical causes situated away from the saphenofemoral junction essentially consist of the presence of a high perforator (5) or a tributary of the arch communicating with the deep pelvic venous network (4).
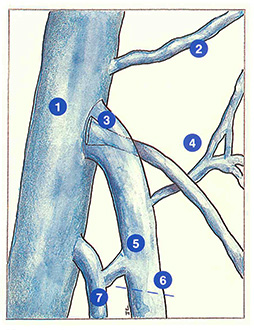
- Hemodynamic causes are due to disturbance of the equilibrium between intravenous pressure and parietal resistance. They are therefore due to either deep iliofemoral venous incompetence (thrombosis, absence of valves) (1), or hypertension associated with parietal hyperdistensibility. This latter situation is usually observed in pregnant women or in individuals with a familial predisposition and with jobs requiring prolonged standing.
“Neo-arches”
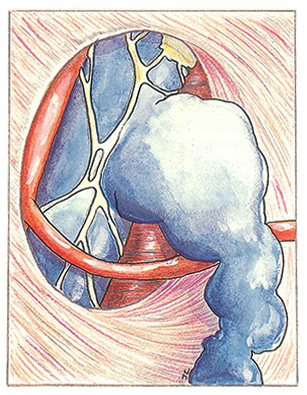
Anatomical causes sometimes lead to the development of what surgeons and ultrasonographers have called a “neo-arch.” This does not correspond to a neoplasm, but to secondary ampullary dilatation of a vein left in place.
Typically, these “neo-arches” arise from a subfascial anterior tributary, often intimately associated with the femoral vein over its last centimetres and terminating in the saphenofemoral angle. Hidden in this way, it may be left in place at the first operation.
Like the saphenous tributaries from which they are derived, the wall of these “neo-arches” is thinner with fewer muscle fibres than the wall of the saphenous vein. Consequently, “neoarches” have a very ectatic and tortuous appearance (Figure 42).
Neovasculogenesis
In this case, the surgeon and ultrasonographer observe a system of venules with fine, fragile walls with a medusa’s head appearance, buried in ‘a cicatricial fibrous tissue. This lesion is sometimes referred to as a “cavernoma.”
These small vessels recanalize an underlying venous trunk, responsible for distant recurrences (Figure 43).
This neovasculogenesis appears to be induced by haemodynamic phenomena, (increased transparietal pressure) and by biochemical mediators responsible for endothelial cell proliferation. Lastly, some authors consider that the development of these lesions may be facilitated by surgical section of the vessel.

Further reading
Waligora J., Frileux C. Les réinterventions pour varices essentielles des membres inférieurs. Société des Chirurgiens de Paris, 1972, 62, 2 : 124-32.
Olivier Cl., Epfelbau R., Dimaria G., Favre M. Les réinterventions pour varices essentielles des membres inférieurs. Presse Med., 1966, 74: 1355-8.
Rettori R. Les récidives variqueuses post-chirurgicales. Phlébologie, 1986, 39, 1: 89-98.
Davy A. Les varices récidivées. Expansion scientifique, 1975, Paris.
Lefebvre-Vilardebo M. Le carrefour anatomique saphénofémoral, source de récidives variqueuses. Phlébologie 89, 1989, i. Libbey Eurotext, 1006-8.