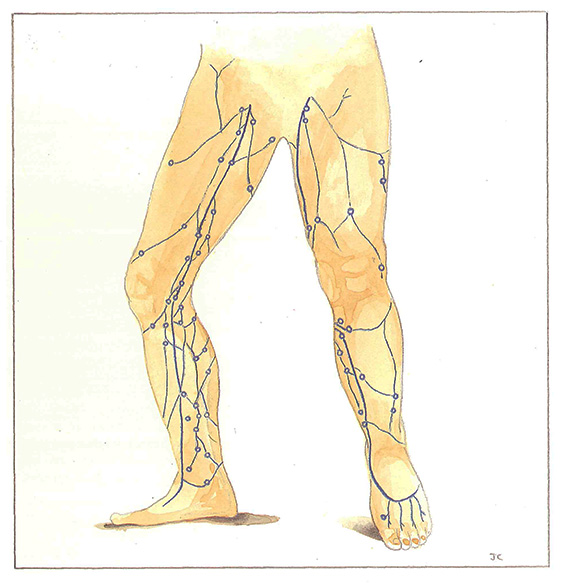
General topography
Rather than describing a perforating vein whose situation is not always as precise and as constant as that described by the author after whom it is named,. it is preferable to define groups of perforating veins (Figures 57 and 58). In general, only one structure of these groups of veins will become pathologically enlarged.

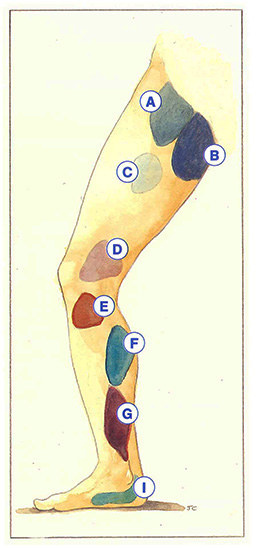
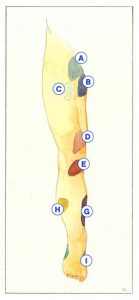
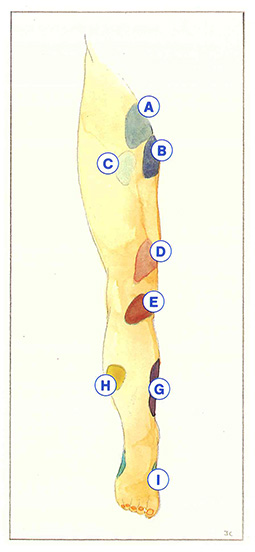
The essential groups of perforating veins are:
- proximal terminal perforating veins (A) which connect the femoral vein with the terminal portion of the long saphenous vein or its accessory veins (upper third of the thigh);
- perineal perforating veins (B) which connect latero-uterine and ovarian veins of the hypogastric network with branches of the long saphenous trunk and its posterior branches, or with the short saphenous network via a Giacomini vein;
- distal terminal perforating veins (C) which connect the femoral vein to the long saphenous network in the middle third of the thigh (main trunk, its accessory veins or tributaries);
- Dodd’s perforating veins or perforating veins of the adductor canal (D) which connect the femoral vein to the long saphenous network in the lower third of the thigh (main trunk, its accessory veins or tributaries);
- Boyd’s perforating veins (E), form a communication between the saphenous network of the subcondylar region of the leg and the popliteal or tibioperoneal trunks;
- medial gastrocnemius perforating veins (F) which communicate between the intramuscular veins of the medial head of the gastrocnemius muscle and the saphenous network of the leg (main trunk, calf plexus, posterior branches). These perforating veins sometimes represent an indirect communication with the short saphenous system, for example via the lower pole vein which travels in the medial head of the gastrocnemius muscle;
- Cockett’s perforating veins (G) between posterior tibial veins and posterior saphenous branches, especially Leonardo da Vinci’s vein;
- peroneal perforating veins (H) connecting the peroneal veins to the anterior saphenous branches;
- perforating veins of the retromalleolar and submalleolar regions (I) forming a bridge between plantar veins and saphenous and marginal branches.
From a pathophysiological point of view, the development of skin lesions is all the more probable, frequent, and severe when the perforating veins involved are situated more distally. Perforating veins of the thigh are usually incriminated in posttreatment recurrences, Boyd’s perforators are involved in the development of varicosities after treatment, medial gastrocnemius perforating veins are responsible for extensive thromboses, and finally, Cockett’s perforators are involved in trophic disorders of the skin.
Further reading
Dodd H., Cockett F.B. The pathology and surgery of the veins of the lower limb. Churchill Livingstone Ed., 2nd Edition, 1976.
Van Limborgh J., Banga D.A., Meijerniks C. Démonstration d’un modèle anatomique des veines de l’extrémité inférieure. Phlébologie 1961; 14: 175.