Accessory saphenous veins
Although the accessory saphenous veins represent a key element in explaining postoperative recurrences, they also participate in the appearance of post stripping varicosities.
It is essential to clearly distinguish between the long saphenous vein, the accessory saphenous vein and tributaries.
An anterior saphenous vein and an anterior tributary of the thigh (anterolateral vein of the thigh) can be distinguished by two main features: structure of the venous wall and topography.
The wall of the long saphenous vein contains a thick media and is referred to as a “saphenous type” of vein wall. The saphenous vein (from the Arabic “safin”: “that which is obvious”) possesses a fairly regularly thickened wall, a wall which is especially “obvious” on palpation, which makes clinical examination all the more important to detect accessory saphenous veins.
In contrast, an anterior tributary has a more fragile wall. Consegtiently, it has a varicose, tortuous appearance with alternating zones of marked ectasia with thin walls and- more rigid zones with a thickened wall.
Topographically, an anterior saphenous vein remains relatively linear and close to the main saphenous vein.
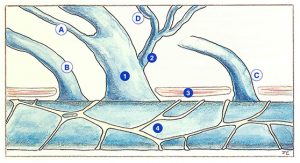
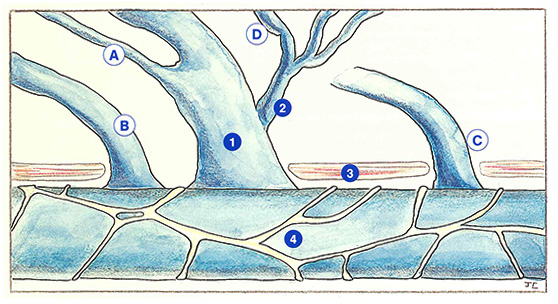
Several types of anastomosis of accessory saphenous veins can be observed (Figure 30). They may drain into the arch of the long saphenous vein (A), directly into the femoral vein below (B) or above (C) the arch, or even into a tributary of the arch (D).
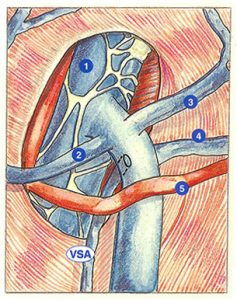
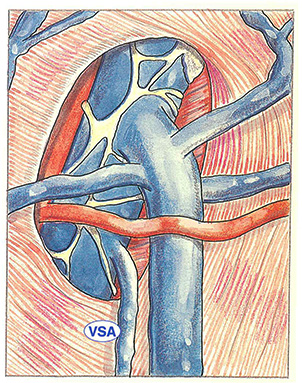
When the accessory saphenous vein drains into the arch of the long saphenous vein (Figure 31), it is unlikely to be missed, except when its anastomosis is situated in the saphenofemoral junction.
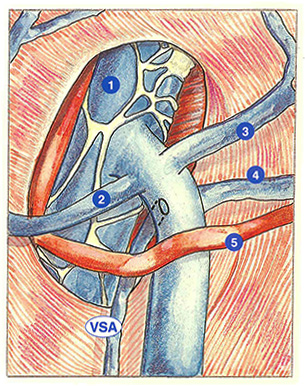
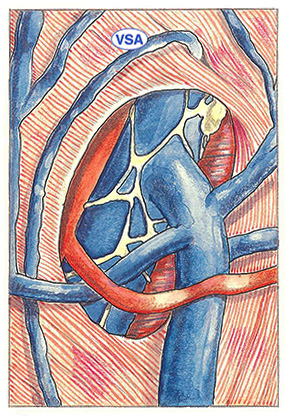
The accessory saphenous vein can anastomose directly with the femoral vein below and independently of the arch of the saphenous vein (Figure 32). This configuration illustrates the absolute necessity of dissection of the femoral vein.
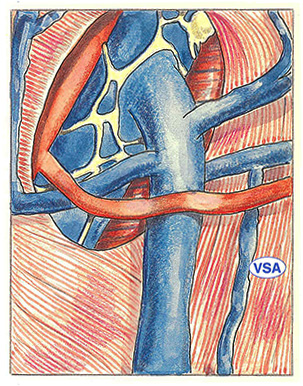
This type of direct anastomosis into the femoral vein can also occur away from the long saphenous vein
(Figure 33).
This type of termination, situated above the saphenous opening, therefore lies outside of the surgeon’s field of vision. This type of accessory saphenous vein may induce varicose disease with an autonomous course. It can also supply a territory of varicosities in the thigh or leg. Such lesions should be treated by sclerotherapy; starting with the highest varicosity.
Finally, always at a distance from the arch of the long saphenous vein, the accessory saphenous vein may sometimes drain into a tributary of the arch, for example an external pudendal vein (Figure 34). If this vein communicates with an intrapelvic vein, an entire varicose network may be supplied independently of a reconstructed saphenofemoral junction.
Further reading
Benhamou A.C. La maladie variqueuse, Arnette Ed., Paris, 1990.
Griton Ph. Que penser des voies de drainage des télangiectasies. Ouest Med, 1985, 38: 603-7.
Vin F. Anatomie du système veineux des membres inférieurs. Artères et Veines, 1983: 383-7.