Short saphenous vein
The relationships of the short saphenous vein with the deep fascia of the leg (fascia cruris) are characterized by their marked variability and their intimate correlations.
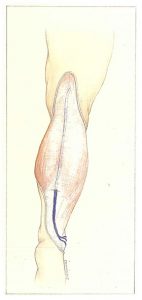
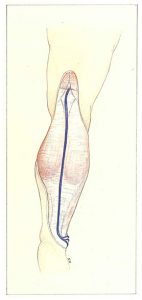
In 60% of cases, the short saphenous vein travels above the fascia in the lower third of the leg. It then perforates the fascia in the middle third of the leg (15 to 25 cm above the lateral malleolus) and continues to ascend underneath the fascia to the saphenopopliteal junction (Figure 82).
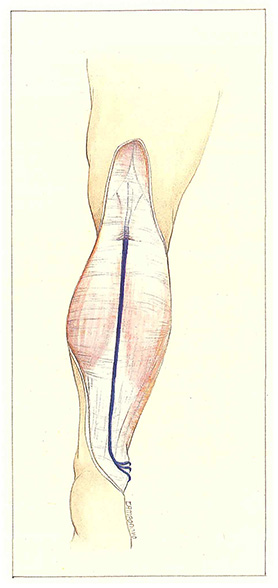
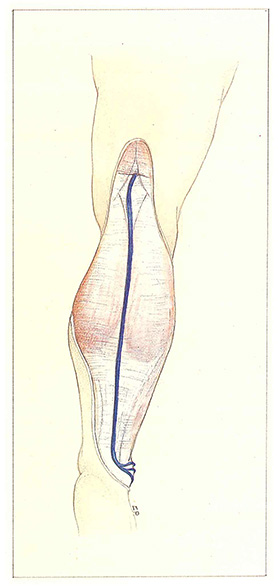
In 30% of cases, the transfascial perforation is situated in the upper third of the leg (Figure 83).
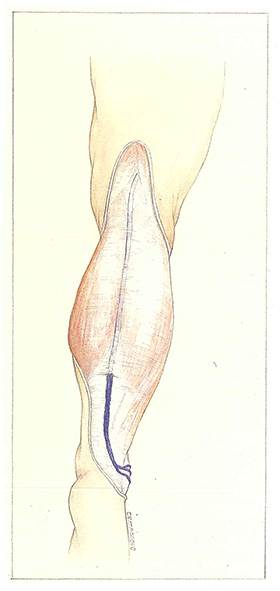
Finally, the short saphenous vein can remain suprafascial as far as the popliteal fossa (4% of cases) (Figure 84)
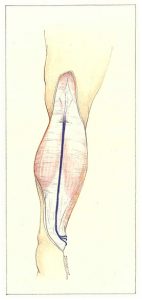
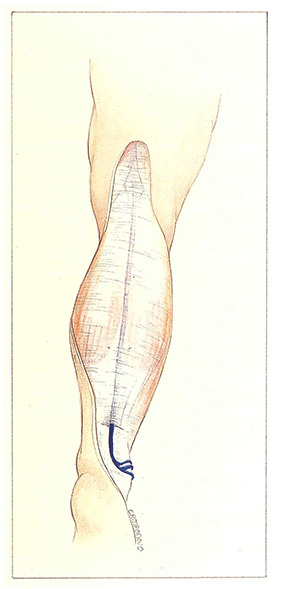
The short saphenous may also perforate the fascia in the lower third of the leg (6% of cases) (Figure 85).

Although the intimate relationships between the fascia and the short saphenous vein are obviously important anatomically, they also have functional implications.
Sedentary subjects, when standing for prolonged intervals, develop excessive muscle tension of the gastrocnemius muscles and limitation of muscle amplitude, well known to physiotherapists. This results in reduction of dorsiflexion of the foot associated with retraction of the fascia cruris continuous with tendo calcaneus. Limitation of muscle contraction and tendon retraction can lead to excess tension on the short saphenous vein or impairment of its drainage, depending on the level of transfascial perforation of the trunk.
In order to more clearly define the functional relationships between the fascia cruris, calf muscles, and the venous network of the leg, we will describe several features of muscle physiology.
Stabilization of the muscles with muscle tension and constant contraction is essential for immobile standing. While standing, the fixed anchor point is represented by contact of the heel with the ground. According to a reverse logic, maintenance of this anchor point implies a constant tension exerted by the calf muscles and hamstring muscles of the posterior surface of the thigh. The consequences on venous physiology are therefore completely different from those observed during walking.
During prolonged standing, the muscle action is ineffective on venous drainage. While walking, the venous pressure in the foot only decreases after the seventh step. All these mechanisms are accompanied by hypertonia of the calf with muscular and fascial retractions. In obese subjects, the tendency to fall forwards induces compensatory contraction of gastrocnemius muscles and worsens the situation. The same applies to patients with plantar postural disorders (eg. pes cavum or high-heeled shoes).
The first consequence consists of ascension of the fascia, which is “drawn” by contraction of the gastrocnemius and hamstring muscles, counteracting the tendency to fall forwards. This situation is observed every day by phlebologists when they detect transfascial passage of the saphenopopliteal junction in a standing patient on duplex ultrasound. This junction is situated somewhat lower in the ventral supine position, as muscle relaxation allows the saphenopopliteal junction to return to its anatomical position.
The second consequence is that the tetanized muscle become fibrotic. resulting in more limited and less effective contraction.
The action of the gastrocnemius muscles on the intramuscular gastrocnemius veins is therefore reflected by the caliber of these veins, but especially by the systolic ejection fraction, which assesses the capacity of the muscle to expel venous blood.
The efficacy of the calf pump simultaneously depends on the quality of muscle fibers, their development by sporting activities. their capacity for stretching and elongation. and finally, the amplitude of their contraction, which can be reduced by a “tetanization”. In this latter case. muscle contraction of this apparently hypertonic calf has little effect on venous drainage.
The situation described above illustrates, once again, that the essential concept of anatomical relations must be considered in the light of functional anatomy.
Further reading
Blanchemaison Ph., Louis G. Relations entre veines, muscles et aponévroses musculaires des membres inférieurs. Phlébologie 1996.