Endoscopic anatomy
Miniaturization of optical fibers has made arteries, and subsequently veins, accessible to investigation “from the inside.” Venous endoscopy has thrown new light on the anatomy and morphology of valves, by studying them in situ.
On endoscopy, the venous wall appears pearly white, smooth, and linear. Venous valves are seen as bicuspid folds derived from the wall and lined by endothelial cells. Between their free edge and their parietal insertion, the two cusps form a space called the valvular sinus, which is concave towards the heart (Figure 8). The parietal edge is thickened and forms the valvular horn. Due to its fibromuscular composition, this thickening constitutes a real sphincter which is able to contract. The free edge of the valvular sinus is also reinforced in the form of a valvular pad. The corresponding horn and pad of each valve define the two valvular commissures.
Several essential features have been confirmed by endoscopic observations.
Not all valves are the same
The long saphenous vein contains 3 to 20 valves. Some of them are reinforced by a fibromuscular skeleton which totally opacifies the valvular cusp. This feature is constantly observed with ostial valves. In contrast, other valves appear transparent with a very fine cusp.

Valves are not located randomly
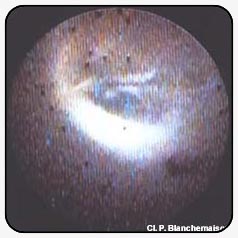
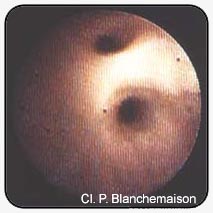
Reinforced valves are always situated in the ostium or directly proximal to the junction of tributaries or perforators (Figures 9 and 10). Their role is therefore not limited to that of a simple antireflux system.
Valves are distributed according to a helical arrangement
This helical arrangement, well known to surgeons who observe it after invagination of the long saphenous vein, appears to be related to the embryological development of the vein. This helical movement is further emphasized by elongation of the varicose vein.
The valves are not distributed homogeneously
In the thigh, the long saphenous vein is usually devoid of valves. Only one or two of the dozen valves of the long saphenous vein are situated above the knee, while the majority of veins are situated distally, in the calf.
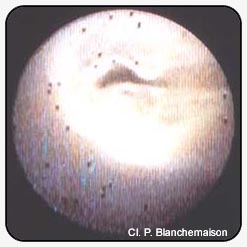
The valves of varicose veins present various types of lesions
These lesions may consist of lengthening of the free edge (Figure 11), fibrous retraction or disinsertion or tearing of a cusp (Figure 12). However, none of these lesions can be attributed to a specific pathophysiological mechanism: parietal degeneration or haemodynamic disorder.

Further reading
Biegeleisen K. Venoscopy as an adjunct to the surgical and non-surgical treatment of varicose veins. In Phlébologie 92, J. Libbey Eurotext, Paris, 1992.
Blanchemaison Ph. Intérêt de l’endoscopie veineuse dans l’exploration et le traitement de l’insuffisance veineuse des membres inférieurs. J Mal Vascul, 1992, 17: 109-12.
Blanchemaison Ph., Griton Ph., Hugentobler JP., Cloarec M. Les valvules ostiales du sujet variqueux. Examen endoscopique. Phlébologie, 1991, 44: 615-22.
Van Cleef IF. Lappareil valvulaire vu en endoscopie veineuse. Vie Med, 1991, 72, 187-90.