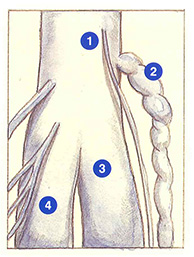
Ectatic gastrocnemius veins

The particular anatomical and hemodynamic characteristics of the veins of the popliteal fossa are responsible for a number of therapeutic difficulties.
Firstly, the anatomical difficulties of this region are related to the confluence of popliteal and saphenous collecting vessels and muscle draining veins.
The hemodynamic difficulties are due to the fact that the popliteal fossa is the site of very intense pressure variations. The intramuscular network constitutes a very large blood reservoir which is suddenly, mobilized during muscle contraction. The pressure within the popliteal network increases considerably in the case of impairment of venous drainage, (postural compression, stretching, and breath-holding effort).
These specific conditions account for the high recurrence rate following saphenopopliteal junction ligation despite a correct surgical procedure, flush with the popliteal vein.
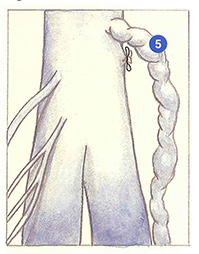
Figure 101 shows a recurrence involving a perforating vein of the popliteal fossa appearing 18 months after saphenopopliteal junction ligation and short saphenous stripping. This type of recurrence is observed all the more frequently when the gastrocnemius veins are ectatic with a large intramuscular blood volume.
In terms of pathogenesis. prior to saphenopopliteal junction ligation, reflux by the short saphenous vein constitutes a sort of safety valve to control hypertension in the popliteal network (Figure 102A).
After saphenopopliteal junction ligation flush with the popliteal vein and short saphenous stripping (Figure 102B), hypertension of the popliteal vein is all the more marked when the gastrocnemius veins are dilated or when there is an obstruction to blood drainage and a new safety valve will he found in the ectatic development of a perforating vein of the popliteal fossa (Figure 102 C).
The rapid development of these recurrences clearly illustrates that the source of venous hypertension and blood reflux is situated in the popliteal region and not in gastrocnemius perforating veins (Figure 102D).


Further reading
Blanchemaison Ph. La physiopathologie veineuse. Phlébologie, 1995; 48: 87-8.
Davy A., Ouvry P. Recurrence of varicose veins. Phlebology, 1986; 1: 15-21.
Hobbs J. The treatment of venous disorders. MTP, Lancaster, 1977: 159-201.
Perrin M. L’insuffisance veineuse chronique des membres inférieurs. MEDSI, Paris, 1990.